Differentiated thyroid cancer is the most common type of thyroid cancer. Positron emission tomography (PET-CT scan) is currently used for the detection of disease which may not be radioiodine avid or as a result of tumor heterogeneity. Tumor heterogeneity is more common in high risk patients and where FDG avid and non-avid disease may co-exist.
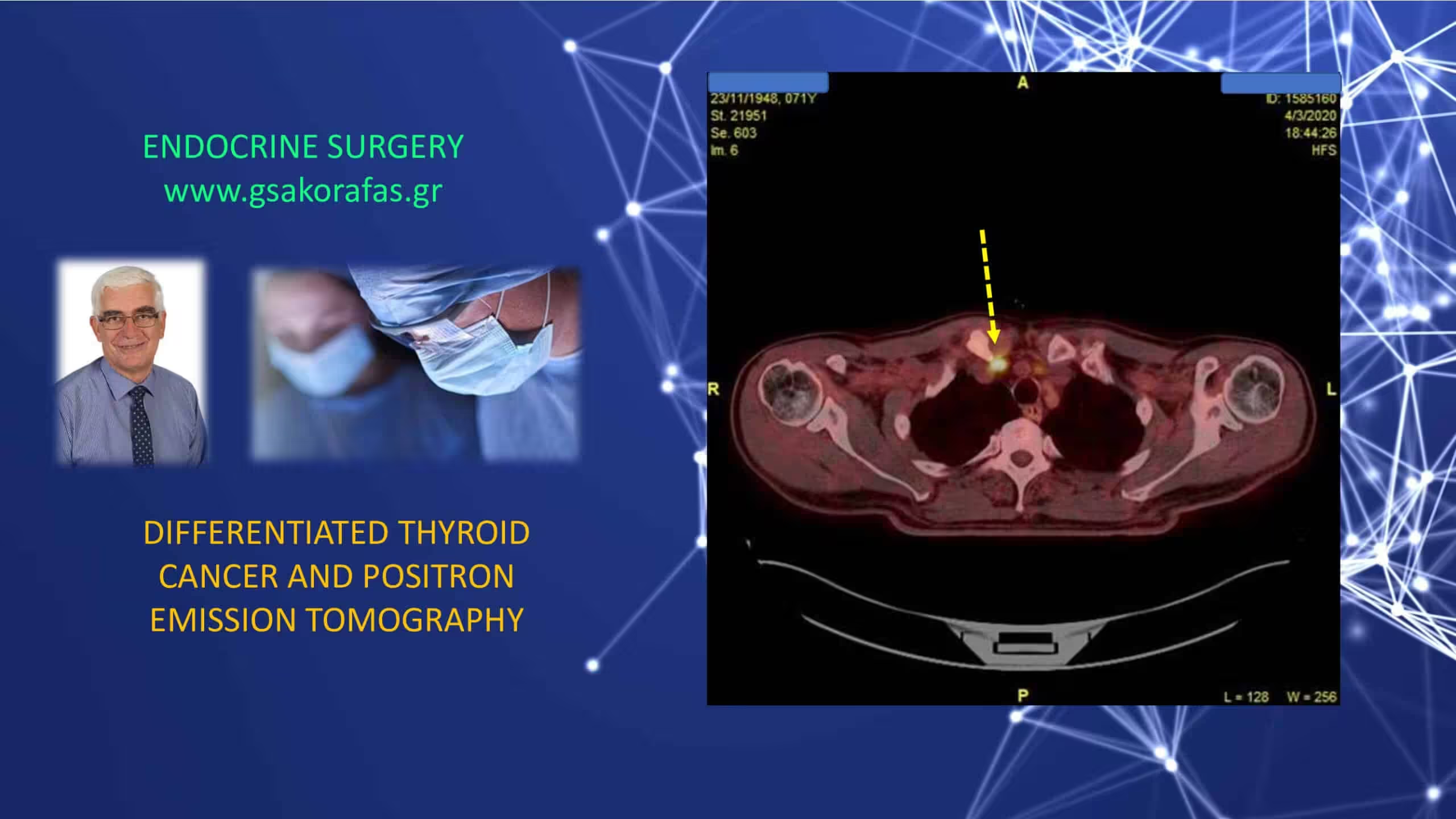
Detection of disease using positron emission tomography
The localization of FDG in differentiated thyroid cancer depends on a number of factors. It is known that GLUT receptors are abundantly expressed on thyroid cells. GLUT1 is particularly found in aggressive variety of thyroid cancer cells. In high risk disease, FDG-PET can:
- identify clinically relevant sites of disease
- assess serially the progress or response to treatment
- identify the need for additional local intervention like EBRT, excision or radiofrequency ablation
- evaluate response to targeted therapies
- help in the staging in high risk patients (advanced T stage, distant metastasis at diagnosis or aggressive histological subtype)
Differentiated thyroid cancer and positron emission tomography – indications
The most common indication of FDG PET-CT scan in differentiated thyroid cancer has been in patients with elevated thyroglobulin levels and a negative radiodine scan.
Another not uncommon indication is the patient with a radioiodine scan not corroborating with the expected disease burden. The disease in this latter group of patientrs undergo gradual de-differentiation with activation of cellular glucose metabolism (the so-called ‘flip-flop’ phenomenon). Currently, it is believed that this phenomenon is not absolute ant that both radioiodine avid and radioiodine refractory (FDG avid) thyroid cancer may coexist in the same patient. FDG PET-CT scan has good sensitivity of detection in this setting, varying between 70 and 90 % in the literature. In specific clinical situations it can affect patient management in 20 – 40 % of cases.
In a recent study (Nucl Med Mol Imaging 50[2]: 130) the sensitivity, specificity, positive predictive and negative predictive values, and accuracy of F-18 FDG PET-CT scan for detecting recurrence were 64 %, 94 %, 86 %, 81 % and 83 %, respectively. False positive results occurred and were due to the presence of reactive lymphadenopathy or postoperative suture granuloma
Differentiated thyroid cancer, positron emission tomography and prognosis
FDG-PET scan provides significant prognostic information. High FDG uptake in metastatic differentiated thyroid cancer is usually seen in de-differentiated, aggressive variety, with poor prognosis and reduced survival. In such cases and high risk differentiated thyroid cancer, total volume of FDG positive disease is the strongest prognostic indicator of survival. Low or no FDG uptake in radioiodine negative disease has better prognosis.
Positron emission tomography and thyroid nodule
The identification of a thyroid nodule on PET-CT scan (usually performed for other indication) has been traditionally associated with an increased risk for the presence of underlying malignancy. However, the rate of malignancy in FDG-avid thyroid nodules is low in the absence of specific suspicious ultrasound features. The SUV values are non-discriminatory to differentiate between benign and malignant cytology. This emphasizes the key role of ultrasonography in the management of patients with thyroid nodules. Further diagnostic investigation (including fine-needle aspiration cytology) may not be necessary in the absence of suspicious ultrasound features.
VISIT OUR WEBSITE![/vc_column_text][/vc_column]